Microvascular Decompression surgery or MVD for Trigeminal neuralgia stands out among all the treatment procedures because it is nerve preserving and addresses the root cause of the problem.
In this section , as in most of the website, we have tried to bring out the detailed replies to questions that our patients or readers want answers for. We have thus aimed to make it as interactive as possible, with the hope that you will find an answer to the question you are looking for. If you have any doubts, or have any queries, please leave a comment below, and we shall try to answer it for you.
What is Microvascular Decompression (MVD) and why is it the best?
The rationale behind this form of treatment is best understood by re-visiting the cause of Trigeminal neuralgia. Then, Microvascular Decompression for Trigeminal neuralgia, becomes the obvious answer.
TN is caused by a compression on the trigeminal nerve by one or more blood vessels (arteries, veins, arterioles, venules, web of blood vessels). The offending blood vessel may be an artery, a vein or both. Occasionally a band of arachnoid (a covering of the brain) is the culprit. Tumors, Multiple sclerosis and other forms of neuropathy may also cause TN.
The Root Entry Zone is the transition zone from brain cells to peripheral nerve cells. This is the zone that is most vulnerable to demyelination by chronic compression.
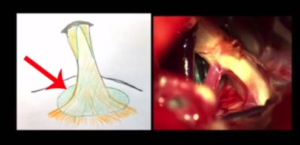
All other procedures which aim to treat Trigeminal neuralgia address the nerve away from the REZ.
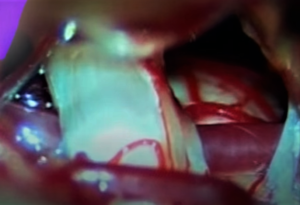
Microvascular Decompression (MVD) is the only procedure that addresses the problem at the REZ. The demyelination-pain cycle is caused by a blood vessel that compresses the nerve. Microvascular decompression separates the blood vessel from the nerve. The neurosurgeon does this by inserting a teflon sponge (most often) between them. This keeps the nerve and blood vessel from not coming in contact with each other.
MVD surgery is the only procedure that achieves a high cure rate that has also the potential to be very long-term and permanent. MVD may also be performed for other cranial nerve hyperactivity disorders like Hemifacial spasms or Glossopharyngeal neuralgia.
How is Microvascular decompression for Trigeminal neuralgia performed?
Microvascular decompression surgery is done under general anaesthesia. A small opening is made behind the ear. The area of the brain where the trigeminal nerve enters the brainstem is exposed. A teflon sponge (a soft pad) is inserted between the blood vessel(s) causing the compression and the nerve.
How is MVD for Trigeminal neuralgia different from that for Hemifacial spasm?
When Microvascular Decompression is performed for treatment for Trigeminal neuralgia, the Trigeminal nerve is identified and decompressed. When MVD for Hemifacial spasm is performed, the seventh nerve is identified and separated from its compressing blood vessel .
Which are the blood vessels that commonly cause compression on the trigeminal nerve leading to neuralgia?
The commonest are arteries, followed by veins. Sometimes it is a combination. The Superior cerebellar Artery (SCA) is the commonest offending blood vessel causing Trigeminal neuralgia. The Anterior Inferior Cerebellar Artery (AICA), the Posterior Inferior Cerebellar artery (PICA), the Superior Petrosal Vein are other notable blood vessels. There could be others as well, but are infrequent.
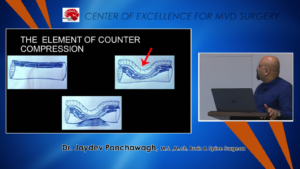
What is counter-compression?
Blood vessels compressing on the trigeminal nerve from one side is ‘compression’.
If the nerve is compressed by blood vessels or other elements from opposite sides, it is called ‘Counter-compression’.
Here is an illustration by Dr Jaydev Panchwagh to explain this concept:
What are the outcomes after Microvascular decompression surgery?
For Trigeminal neuralgia treatment, Microvascular decompression offers the greatest chance of long-term pain relief with permanent cure in a very high number of patients.
Is MVD useful in treating trigeminal neuralgia caused by multiple sclerosis?
Unfortunately, anti-convulsants and other medications are not very effective in multiple sclerosis. Of all the ‘surgical’ procedures that are performed for treating TN, MVD is the only nerve-preserving one. Nerve-destroying procedures may also be performed depending on the stage of the disease. Recurrences are not uncommon, as all treatments are likely to be of limited use.
Is Microvascular decompression of use in atypical Trigeminal neuralgia?
It is of use, for sure, but has a slightly lesser chance of success than in classical TN.
How long does Microvascular decompression surgery last?
MVD surgery lasts about four hours from the time anaesthesia is induced till about the patient is woken up. Of course, there are small variations depending on the patient’s medical profile.
Is Microvascular decompression safe?
MVD is a surgical procedure. There are some inherent risks associated with Microvascular decompression surgery, like any other surgical procedure,. But with technical advances and improving techniques, Microvascular decompression surgery has become safer than in the last decade, even.
Another very important choice that makes MVD safer, is to get operated by an experienced neurosurgeon. The more the number of surgeries one has performed, the better are the results. The surgical team also is well-prepared.
Dr Jaydev Panchwagh is a neurosurgeon renowned for his dedication and commitment to getting the best results in Microvascular decompression surgery. He and his team work hard in synchrony to achieve this. This is one of the reasons why he has many outside-state Indian, and international patients visiting him.
Does Microvascular decompression work?
Yes!! The person who performs the procedure and patient selection are two very important criteria deciding success. At Dr Jaydev Panchwagh’s MVD centre, success rates are in the range of 97-98%.
Who can undergo Microvascular decompression surgery for treatment of trigeminal neuralgia?
The first line of treatment for TN will be medications like anti-convulsants and others.
Indications for MVD at our centre are:
- patient’s pain not well-controlled on medication
- the side-effects of medication become unbearable
- allergy to medication
- non-compliant with medication for various reasons
- classical TN in young and middle-aged and otherwise fit patients early on in the disease
- other failed procedures
- type 2 TN, TN caused by Multiple sclerosis etc after in-depth counselling
Which is the best treatment for Trigeminal neuralgia?
Microvascular decompression is. This is because it fixes the underlying cause.
How is the recovery after Microvascular decompression surgery?
MVD surgery is done under general anesthesia. It takes about 2 to 4 hours to recover from the after-effects of anaesthesia. There will be some stiffness in the neck muscles for a few days after the operation. This gradually reduces on gentle neck movements.
Some patients may experience dizziness for a couple of days. Patients are made to stand by the bedside on the first day after operation, and encouraged to walk short distances on the second day (depending on fitness). Gradually these distances may be increased. Full activity is allowed only after about 6 weeks or later, after the neurosurgeon gives the go-ahead.
Pain-killers and antibiotics may induce some amount of nausea. Appropriate dietary modifications and other medication may help.
Can Microvascular decompression completely cure the pain of trigeminal neuralgia?
No surgery promises hundred percent results. So is Microvascular decompression surgery. In majority of the patients the facial pain disappears on waking up from operation. Recurrences are rare, but are possible, at a later date.
Is Microvascular Decompression surgery used for any other disease treatment?
Yes, MVD surgery is also performed for treatment of Hemifacial spasm or Glossopharyngeal neuralgia. Rarely it is also used to treat very specific types of tinnitus.